
Scientific Calendar May 2023
Urinary cellular atypia in bladder cancer surveillance
Why is post-treatment surveillance for bladder cancer patients unavoidable?
Bladder cancer occurs only one time.
Bladder cancer is a highly recurrent kind of cancer.
Symptoms appear early and are sufficient for cancer surveillance.
Sonography is enough for bladder cancer surveillance.
In the first year after treatment, quarterly cystoscopies are required.
Cystoscopies are a convenient procedure for patients.
Congratulations!
That's the correct answer!
Sorry! That´s not completely correct!
Please try again
Sorry! That's not the correct answer!
Please try again
Notice
Please select at least one answer
Scientific background
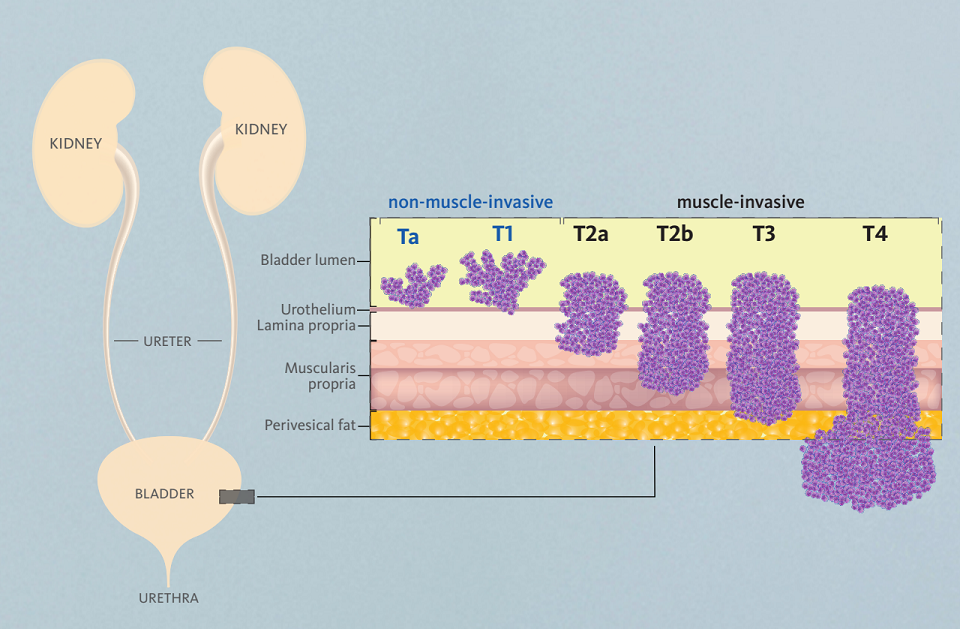
Bladder cancer is a malignant disease that originates from the epithelial cells of the urothelium of the bladder. Bladder cancer is distinguished using two main groups: non-muscle-invasive and muscle-invasive bladder cancer (Fig. 1).
Non-muscle-invasive bladder cancer includes the stages 0 and 1 and manifests as a spread within the urothelial layer (carcinoma in situ) or as a polyp-like structure that outgrows from the urothelium into the lumen of the bladder. From stage 1, the tumour also spreads into the Lamina propria.
Muscle-invasive bladder cancer includes the stages 2 to 4 and spreads further into the different layers of the bladder. In stage 2, the muscle layer Muscularis propria is affected, in stage 3, the perivesical fat layer is affected, and in stage 4, the tumour spreads into blood vessels and metastasizes into other tissues.
Smoking is the main cause for bladder cancer, accounting for 65 % of cases in male and 30 % of cases in female individuals, respectively. Additional drivers of bladder cancer include exposure to chemical substances, especially aromatic amines, a medical and family history of bladder cancer, previous cancer treatment, and recurrent bladder infection especially with Schistosoma haematobium.
Bladder cancer is the fourth most common type of cancer in men, predominantly affecting men of Caucasian ethnicity at the median age of 69 years. In females, the prevalence is much lower, affecting females at a median age of 71. However, changing lifestyles lead to a decline of the median age and an increased number of cases in female individuals.
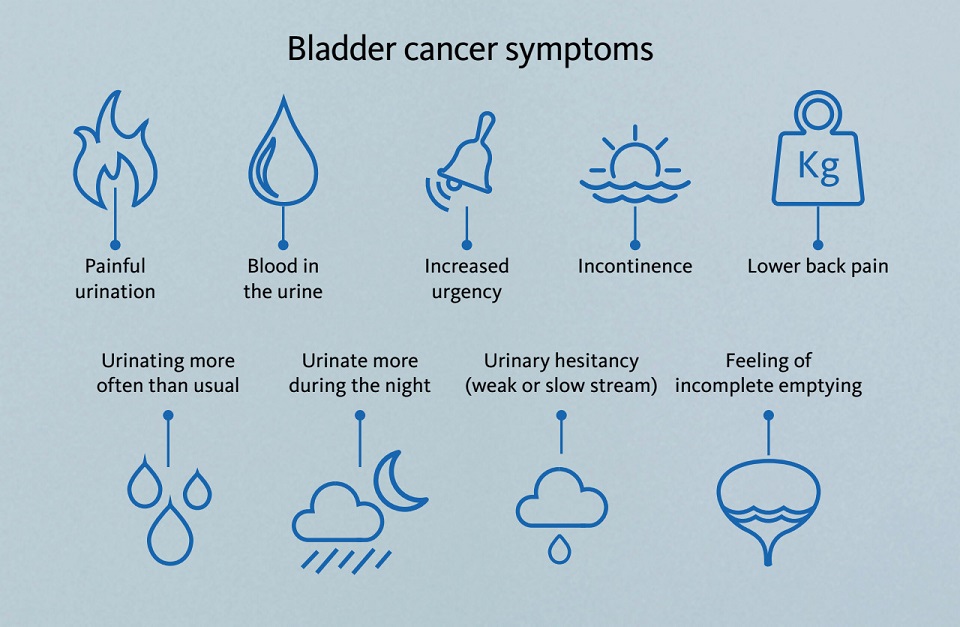
Symptoms are largely unspecific and resemble those of other disorders of the urinary tract, such as urinary tract infections or urolithiasis, including dysuria, pollakiuria, lower back pain and haematuria (Fig. 2). Thus, there is the risk to misinterpret symptoms. However, gross haematuria, leading to macroscopic visibility of blood in urine is the most common symptom, driving diagnostics that lead to the diagnosis of bladder cancer.
The overall survival of bladder cancer strongly depends on the stage of the tumour at the time of diagnosis: The five-year survival rate declines from 98 % at stage T0 and 88 % at stage T1 down to 15 % at stage T4 (Fig. 3).

The main diagnostic tool for the diagnosis of bladder cancer is cystoscopy, which is an invasive, unpleasant and time-consuming technique, and due to the low prevalence of bladder cancer not suitable as a screening tool for the population at risk. Additionally, urine cytology and other biomarkers, such as BTA and NMP22, might be of interest, but show diverse performance.
Bladder cancer is a disease with a high rate of tumour recurrence of 60 % within the first year and 80 % within five years after treatment. Therefore, active and frequent surveillance of known bladder cancer patients by cystoscopy is mandatory, once per quarter in the first year after treatment and one to two times annually in the following years.
Atypical cells – cells that are suspicious of being malignant – are a target of urine cytology to support the detection of bladder cancer. With the research parameter Atyp.C, the UF-Series has the potential to detect atypical cells in urine samples within the scope of routine urinalysis.
The patient case
Two years ago, a 77-year-old male patient underwent chemotherapy and trans-urethral resection (TURBT) of a stage one, non-muscle invasive bladder cancer (NMIBC). The post-treatment surveillance now includes half-yearly follow-up examinations because of the high risk of tumour recurrence.
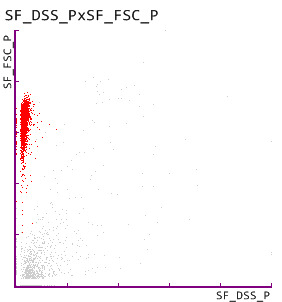
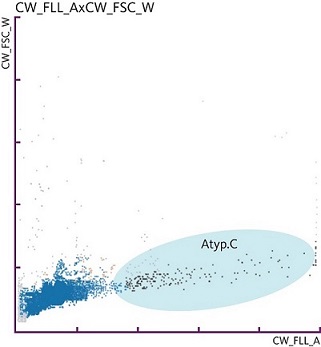
Recently, the patient has been suffering from fatigue and pollakiuria. An initial routine urinalysis examination revealed the presence of 2,956 RBC/µL that were characterised as isomorphic RBC, indicating a macrohaematuria of non-glomerular origin (Fig. 4). In addition, 3.9 atypical cells per µL were detected, as highlighted by the research parameter ‘Atyp.C’ (Fig. 5), suspecting the presence of malignant cells.
Based on these findings, an extraordinary cystoscopy was requested, leading to the detection of a recurrent, papillary urothelial carcinoma. This highlights the potential of the Atyp.C research parameter to support bladder cancer surveillance.
Depicted in the calendar image: bladder cancer relapse
The image shows the lumen of the bladder with the base of the urethra in the centre. The urothelium of the bladder shows several papillary structures, representing early stages of recurrent bladder cancer. In addition, horseshoe-shaped tissue alterations show areas where transurethral resections previously took place.

References
[1] Karaburun MC et al. (2023): Investigation of Atypical Cell Parameter in the Surveillance of Patients with NMIBC; Initial Outcomes of a Single Center Prospective Study. J Med Syst. 47(1):41. [abstract]
[2] Aydin O (2021): Atypical cells parameter in Sysmex UN automated urine analyzer: feedback from the field. Diagnostic Pathology. 16:9. [open access]
[3] Ren C et al. (2020): Investigation of Atyp.C using UF-5000 flow cytometer in patients with a suspected diagnosis of urothelial carcinoma: a single-center study. Diagn Pathol. 15(1):77. [open access]
[4] Tınay İ et al. (2020): “Atypical Cell” Parameter in Automated Urine Analysis for the Diagnosis of Bladder Cancer: A Retrospective Pilot Study. Bull Urooncol. 19(1):17–19. [open access]
[5] Aydin O et al. (2020): Atypical cells in Sysmex UN automated urine particle analyzer: a case report and pitfalls for future studies. Turk J Biochem. 45(5):617–619. [open access]
