
Scientific Calendar November 2021
How high would you estimate the lethality in patients with systemic candidiasis?
Less than 10%
Between 20 and 30%
Up to 50%
More than 80%
Congratulations!
That's the correct answer!
Sorry! That´s not completely correct!
Please try again
Sorry! That's not the correct answer!
Please try again
Notice
Please select at least one answer
Scientific background
Immunocompromised and weakened patients such as cancer patients under chemotherapy are often threatened by hospital-acquired infections. Common causes for the so-called ‘nosocomial’ infections are fungi, especially Candida albicans or other Candida subspecies [1].
Normally, Candida spp., which belong to the family of yeasts, colonise the skin and mucosa and do not cause harm in healthy individuals. On the contrary, in immunocompromised patients Candida spp. can overgrow and enter the bloodstream, leading to severe invasive infections and the patients are likely to deteriorate into sepsis if not treated timely. Moreover, the yeasts often form biofilms on catheters or other intravenous entry points, allowing the microorganism to enter the bloodstream of the host. Interestingly, fungal sepsis is associated with higher lethality (up to 50%) than bacterial sepsis [1, 2] and is therefore considered a serious healthcare burden associated with high costs.
Neutrophils have been described to have an ambivalent function in fungal sepsis patients [2]. They orchestrate the innate immunity which help fight the invading pathogen. Nevertheless, their potent ability to activate the immune system is a key trigger of the development into sepsis and septic shock. Neutrophils express recognition receptors for the yeast and the hyphae and can also form extracellular chromatin nets to trap the fungi. On the other hand, monocytes, the second most abundant cells of the innate immunity, do not show comparable potent antifungal activity [2].
Typically, antifungals such as fluconazole are administrated after a positive blood culture for Candida spp. The rising numbers of resistant non-albicans strains such as resistant Candida auris are becoming a severe threat. Hence, the performance of a respective antibiogram is recommended and the importance of antibiotic and infectious disease stewardship programs is underlined once again [3].
Numerical results
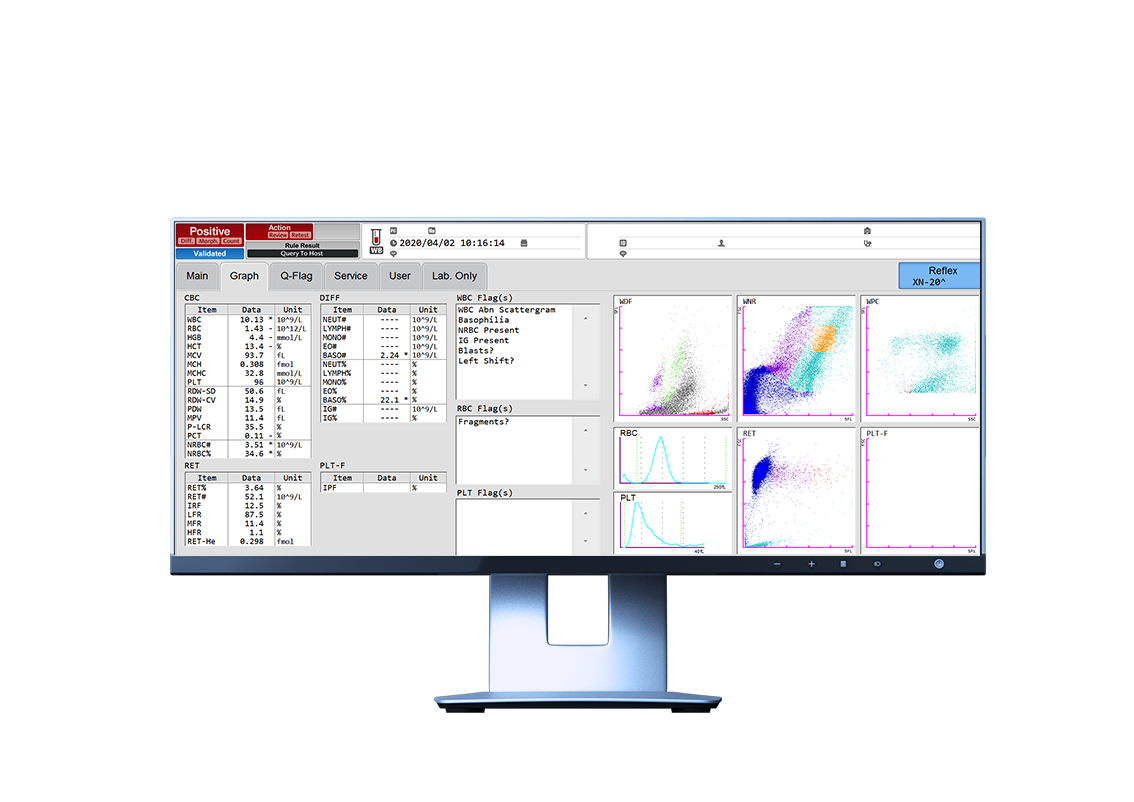
The first measurement of a patient’s blood on the XN-Series analyser revealed a normal white blood cell count (WBC 10.13 x 109/L), anaemia
(RBC 1.43 x 1012/L, HGB 7.9 g/dL or 4.4 mmol/L) and thrombocytopenia (PLT 96 x 109/L).
Looking at the WNR, WDF and WPC scattergrams, a strong interference can be noticed. Abnormal clouds were detected on the left side of the WNR scattergram around the debris area (dark blue) and were partially misclassified as nucleated red blood cells (NRBC). In the WDF scattergram, the separation of lymphocytes and monocytes are somewhat normal, but an interference occurred between the debris and neutrophil area, not allowing for any clear separation. Consequently, the analyser triggered the message ‘WBC Abn Scattergram’ and the numerical data for the differential was not provided. In such situations, a blood smear should be performed and reviewed.
Although the analyser is not designed to pick up fungi, the smaller and less granular shape of the yeasts as compared to WBC justifies their localisation on the scattergrams, approaching the hypothesis of possible systemic yeast infection [4].
It was also reported in the past that yeast may influence the results of haematology analysers only when the fungi concentration is unusually high. However, it was later concluded that the results differed among analysers and species of yeast [5].
The blood culture of this patient was tested positive for Candida albicans and the treatment with fluconazole started accordingly. A control performed later the same day already showed normal WNR and WDF scattergrams. The patient’s situation improved without fever after three days of treatment, and normal blood gas analysis and negative blood culture could also be observed.
Scattergram interpretation
The careful observation of all the information provided by the automated blood count, including the thorough analysis of the scattergrams of the WBC populations, launches as a promising tool for the diagnostic support and monitoring of the patient [6].
References
[1] Cheng MF et al. (2005): Risk factors for fatal candidemia caused by Candida albicans and non-albicans Candida species. BMC Infect Dis 5:22.
[2] Duggan S et al. (2015): Host response to Candida albicans bloodstream infection and sepsis. Virulence. 6(4):316–326.
[3] https://www.cdc.gov/fungal/candida-auris/index.html, visited 21 September 2021.
[4] Gérard D et al. (2020): Abnormal dot plots on current automated blood cell analyzer helped to yeast detection. Clin Case Rep. 8:776–777.
[5] Kim HR et al. (2008): Effects of bacteria and yeast on WBC counting in three automated hematology counters. Ann Hematol. 87:557–562.
[6] Comar SR et al. (2021): Early detection of Candida parapsilosis sepsis in peripheral blood as a result of cytografic changes on the Sysmex XN-3000 hematology analyzer. Int J Lab Hematol. 00:1–4.



